Australia’s frontline workforce carries a level of psychological strain that extends well beyond what existing systems capture, with most distress remaining unreported and unaddressed despite its scale. Current reliance on compensation data obscures the true extent of the problem, masking the structural drivers, from job design to time pressure, that are shaping mental health outcomes across essential services.
Australia’s frontline workforce has always been defined by its willingness to step forward when others step back. In hospitals, emergency services, schools, and public safety roles, people show up to absorb pressure, trauma, and uncertainty on behalf of the rest of us. However, that expectation comes at a cost.
Across Australia, millions of frontline workers are carrying ongoing psychological distress, and most of it is unreported, unsupported, and largely invisible to the systems designed to protect them.
What the latest research makes clear is that this is no longer a peripheral issue. It is systemic, measurable, and deeply embedded in how frontline work is structured and experienced, and, crucially, it’s not being captured by the metrics we rely on. The problem we are measuring is not the problem we are living.
For years, workplace mental health has been viewed through the narrow lens of workers’ compensation claims. It’s a convenient metric because it’s visible, quantifiable, and tied to cost. However, as Keith Govias, a workplace safety and risk principal at EML Group explains, this lens captures only a fraction of what is actually happening.
“We’ve been looking at mental health through workers’ compensation statistics, but what we didn’t have was the context of mental health as a continuum,” he says.
The Monash Healthy Working Lives Research Group—through the work of Professor Alex Collie, Dr Michael Di Donato, and biostatistician Luke Sheehan—collaborated with EML Group to close that gap. By analysing four major national datasets, they reframed the issue entirely and the result, published in the whitepaper, Inside the minds of Australia’s workplaces: Evidence, insight, and collective action for better mental health outcomes, is stark.
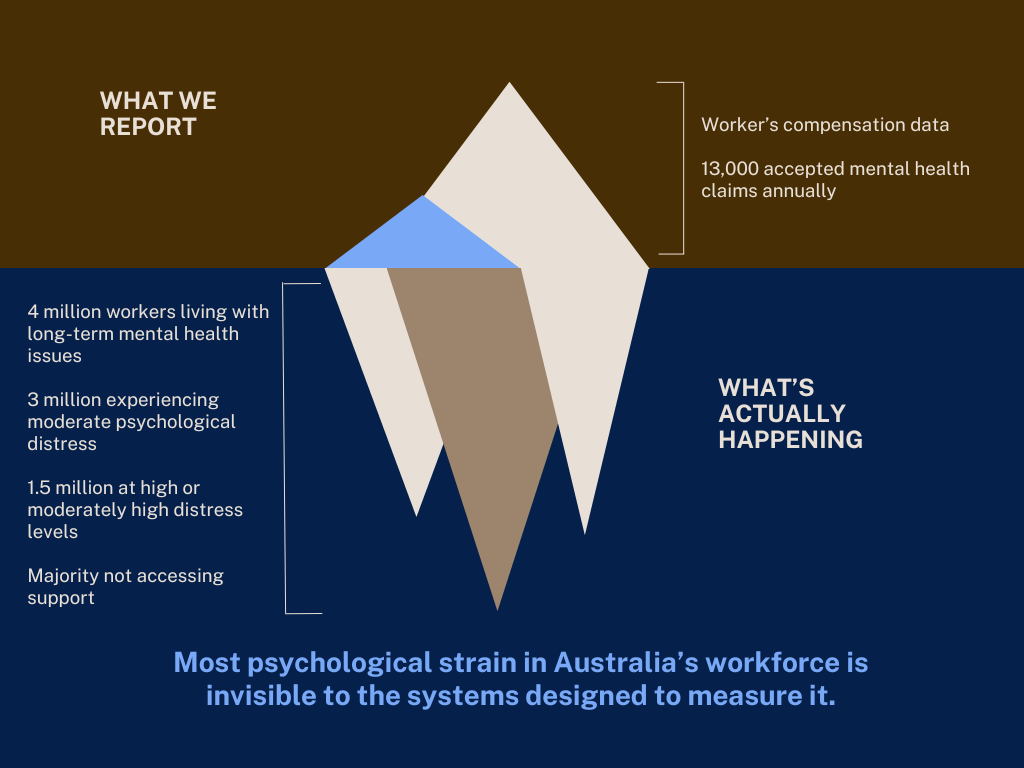
While around 13,000 mental health claims are accepted annually, more than four million Australian workers report living with a mental health condition lasting six months or more. That is a conversion rate of just 0.3 per cent. Even though only a fraction of those four million people will have a work-related mental health condition that would make them eligible for workers’ compensation, there is a deeper insight that lies beneath that number.
Around three million workers are experiencing moderate psychological distress, while at least 1.5 million are already at high or very high levels, which is equivalent to a diagnosable condition. Even worse, despite one in 10 workers with a physical injury claim reporting severe psychological distress, three in five had not accessed a mental health service in the past 12 months.
In other words, the vast majority of psychological strain is not only unclaimed, it’s already embedded across the workforce, often co-existing with other forms of injury and going largely unaddressed.
Govias unpacks this as the iceberg problem. What organisations measure is only the visible tip. What workers experience is everything below the surface.
The frontline reality of pressure, trauma, and accumulation
For frontline workers, mental health challenges are cumulative, embedded in the nature of the job, and often normalised as part of “just doing the work.” Monash’s data reinforces what many already know intuitively.
Emergency services workers are twice as likely as the general population to develop mental health conditions, with one in 10 developing PTSD following critical incidents. Healthcare, public administration, and education collectively account for 62 per cent of all mental health claims.
But statistics alone do not capture the lived experience. Frontline work is defined by repeated exposure to trauma, conflict, emotional labour, and responsibility without always having control. Over time, this creates what researchers increasingly describe as cumulative psychological load.
“Our understanding has evolved,” says Govias. “Early efforts focused on connecting injured workers to treatment, but with more than 100,000 emergency services personnel supported through complex recovery journeys, a clearer picture has emerged and it’s pointing upstream. This isn’t just a workers’ compensation problem. It’s a public health problem and we need to move the conversation from response to prevention.”
Why the system is struggling to keep up
If the scale of the problem is now clearer, the next question is why existing systems are failing to keep pace. Part of the answer lies in how mental health manifests in frontline roles.
Unlike physical injuries, psychological injuries are often delayed, diffuse, and harder to diagnose. They also take longer to recover from. PTSD claims can keep workers off the job for close to a year, while other mental health conditions regularly result in months away from work.
At a system level, this translates into significant workforce loss. In healthcare alone, the equivalent of roughly 2,000 full-time workers are lost each year due to mental health conditions. Across frontline sectors more broadly, the cumulative impact runs even deeper.
There is also a persistent treatment gap. While support structures may exist, access and utilisation remain uneven. More than one-quarter of workers experiencing severe psychological distress do not access mental health services at all.
“Frontline personnel often do not receive evidence-based PTSD treatment,” Govias explains, reflecting on earlier system shortcomings.
This has begun to change. The development of specialised PTSD guidelines, which are grounded in systematic evidence and updated with real-world data, has improved outcomes significantly, with recovery rates reaching around 80 per cent in supported programs, well over the global average of 50 to 60 per cent. However, treatment alone cannot solve a problem that is structural.
The hidden drivers of job quality, time, and culture
One of the most important contributions of the Monash research is its focus on psychosocial job quality. Mental health outcomes are not just about exposure to trauma. They are shaped by the everyday conditions of workload, autonomy, support, and predictability.
Across the workforce, 70 per cent of workers are exposed to at least one form of poor psychosocial job quality. In frontline sectors, these pressures are often intensified.
The most common drivers of psychological injury are not surprising, but they are significant. Workplace bullying and harassment account for the largest share of claims, followed closely by work pressure and exposure to traumatic events. Together, these factors point to a system where risk is not incidental, but embedded in how work is structured.
There are also demographic dynamics at play. Younger workers are entering the workforce already reporting high levels of distress, while older workers are more likely to lodge claims, often after longer periods of accumulated strain. Gender adds another layer of complexity. Women experience significantly higher rates of working years lost and claim frequency, while men tend to experience longer durations and more severe stress during claims.
All of this points to the more complex reality that mental health is not a single issue. It’s an interaction between work design, workforce composition, and cultural expectations.
One emerging but under-discussed factor is time. Frontline workers are not just managing demanding roles. They are navigating what could be described as time poverty, which is the inability to recover, decompress, or access support because of workload, shift patterns, and life responsibilities.
This is where organisational intent often collides with operational reality. Support exists, but time to use it does not.
Shifting from response to system design
If the problem is systemic, the solutions must be too. The research and field experience point to several interventions that consistently improve outcomes.
The first is early intervention, with the report noting that it delivers better outcomes and faster recovery. This is not just about clinical care, but identifying distress before it escalates into injury through better visibility, more proactive management, and a cultural shift away from waiting until someone is unwell enough to step away.
The second is evidence-based treatment pathways. Specialised, trauma-informed care—delivered by clinicians who understand frontline contexts—has been shown to significantly improve recovery rates.
This is followed by peer and organisational support. “International research highlights the effectiveness of peer-led models like Stress First Aid, as well as organisational approaches that address cumulative stress and moral injury. These concepts are already being applied globally, with measurable impact,” says Govias.
However, perhaps the most important shift is in how organisations design work itself. Mental health cannot be treated as an add-on. It must be embedded into job design through manageable workloads, clearer roles, supportive leadership, and environments where psychological safety is actively maintained.
From resilience to responsibility
For years, the dominant narrative around frontline mental health has been resilience, focusing on building stronger individuals, providing tools, and encouraging self-care.
These are important, though incomplete. The evidence suggests that resilience cannot compensate for systemic strain, and must be matched by organisational responsibility.
“The data must inform our strategies and our collective approach, and this means shifting from asking how individuals cope to asking how systems support them,” says Govias.
It also means recognising that mental health is not just a workforce issue, but a societal one. The functioning of healthcare, emergency services, and public systems depends on the wellbeing of the people within them.

Where to from here
The path forward is not about a single intervention. It is about building systems that reflect the true nature of the problem.
There are five important next steps:
- Organisations need to rethink how they measure mental health. Workers’ compensation data alone is no longer sufficient. A more complete view—one that captures distress across the continuum, including those who never lodge claims—is essential to understanding risk early and responding effectively.
- Early intervention must move from principle to practice. The evidence is clear that earlier support leads to better outcomes, but this requires systems that can identify, respond, and act before distress escalates into injury.
- The design of work itself must change. The drivers of psychological harm—work pressure, bullying, and repeated exposure to trauma—are not peripheral issues, they are structural. Addressing them requires deliberate redesign of roles, workloads, and support systems, not just additional services layered on top.
- Responses must become more targeted. The data shows clear differences across industries, genders, and career stages. A one-size-fits-all approach will not be effective. Strategies must reflect the specific risks and realities of different workforce groups.
- Finally, this must be understood as a workforce sustainability issue. When thousands of frontline workers are lost each year to mental health conditions, the impact extends beyond individuals. It affects system capacity, service delivery, and the resilience of essential services themselves.
The iceberg is no longer hidden, because the data has made it visible. The opportunity now is not just to respond, but to redesign the systems that created it, before more of it surfaces.