Menopause introduces significant physiological and psychological changes that can disrupt performance, recovery, and overall wellbeing, particularly for women accustomed to maintaining high levels of output across multiple areas of life. These shifts are often misunderstood or misdiagnosed, despite their broad impact on physical health, cognitive function, and workforce participation, highlighting the need for greater awareness and more tailored approaches to support during this transition.
For high-performing women used to pushing their minds and bodies through balancing family, career, fitness, and service, the transition to menopause can make it feel harder to hold it all together. That’s because it represents one of the most significant hormonal shifts in a woman’s life, and is comparable to puberty and pregnancy.
From about the age of 45, women enter menopause when menstruation permanently ceases for 12 months and the reproductive system no longer performs fertility functions. Perimenopause is the transitional phase leading into menopause, typically lasting between four and eight years. Menopause occurring before the age of 40 is considered premature and can result from surgery, chemotherapy, radiotherapy, ovarian failure or removal.
Symptoms can vary between women as they transition; however, the most common are: hot flashes, night sweats, vaginal dryness, insomnia, trouble focusing, changes in body composition, and mood swings. While blood and urine tests can be carried out to detect changes in hormone levels, experts warn that symptoms should not be ignored, as they often signal the need for a fundamental shift to new strategies for training, recovery, diet, hormone therapy, sex, and sleep.
The physiological changes no-one prepared you for
Despite the inevitable onset of menopause, the decline in sex hormones can take many women by surprise. These hormones regulate far more than just reproduction, influencing muscle mass, bone density, insulin sensitivity, inflammation, and how the body uses fuel during exercise.
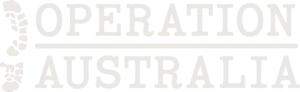
As women’s oestrogen declines, several things occur simultaneously:
- muscle protein synthesis becomes less efficient
- the body becomes more insulin resistant
- fat storage shifts toward the abdomen
- recovery from high-intensity exercise slows
- stress responses become more pronounced.
Dr Mary Claire Haver, an obstetrician-gynaecologist and menopause specialist, says menopause occurs when the ovaries stop producing significant levels of sex hormones, primarily oestrogen and progesterone, along with smaller amounts of testosterone. Dr Haver warns that menopause cannot be diagnosed solely by the textbook definition of 12 months without a period. Factors such as hysterectomy, IUD use, endometrial ablation, and conditions like polycystic ovary syndrome (PCOS), can obscure that marker, contributing to misdiagnosis, and, in some cases, women being prescribed antidepressants in place of hormone replacement therapy (HRT).
Dr Haver explains that hormonal changes can be highly unpredictable at the onset of perimenopause as the body is trying to rebalance against a declining egg supply. For many women, this can present as heavy or debilitating periods, significant fatigue, and a cluster of symptoms that are vague and easily attributable to other conditions, which continues delays in diagnosis.
“The musculoskeletal system takes a huge hit through the transition, so, all of a sudden, you have no injury and you’re having hip pain, joint pain, back pain with, you know, you go to the doctor and you get an x-ray, you do whatever work up, and they can’t find anything wrong,” Dr Haver told the Huberman Lab.
“Palpitations are huge—along with hot flashes, palpitations—so a woman will walk into the emergency room sweating profusely, horrible palpitations, she’s got anxiety, and they’ll tell her she’s having a panic attack. No-one knew to connect the dots and figure out that this woman was in her menopause transition, and this is how her body was expressing it.
“We end up with this very volatile curve, not predictable at all, [that] we call the zone of chaos; it is literal hormonal chaos. What used to look like this, you know, every month is now just insane and very, very, very unpredictable,” Dr Haver said.
The brain is particularly very sensitive to these shifts as fluctuations in oestrogen, progesterone, and testosterone disrupt key neurotransmitters, including serotonin and dopamine. In the United States, the menopause transition has been linked to a 40 per cent increase in mental health disorders, a doubling of SSRI use, and one in five women leaving the workforce.
Emerging evidence suggests that women prescribed HRT during perimenopause experience lower rates of depression, prompting some clinicians to call for greater consideration of oestrogen therapy rather than defaulting to antidepressants.
Dr Stacy Sims, an exercise physiologist and nutrition scientist specialising in female performance, encourages women to better understand and respond to the signals their bodies are sending, stressing that perimenopause is a normal and universal transition for those who have had a menstrual cycle.
“Women have a definitive point in our late 40s, early 50s, where all of a sudden, things go to shit,” Dr Sims told Huberman Lab.
“I think I would have everyone understand their intrinsic selves because we have been inundated so much with sociocultural rhetoric, and so much external noise, that women have forgotten what it means to listen to themselves and their bodies.”